INTRODUCTION
Osteoporosis can cause bones to be easily fractured by small shocks from outside due to a reduction in bone mass and a change in the microstructure of the bone. That is one of the most common metabolic bone diseases. Women are more likely to develop this disease. This is for the following reasons. Firstly, their peak bone mass is lower than that of men. Secondly, after menopause, deficient secretion of estrogen caused by ovarian dysfunction makes the function of osteoclasts hyperactive. This leads to rapid bone resorption and osteoblastic cell impairment. As a result, bone loss progresses gradually [1]. It is important to note that bone fractures from osteoporosis appear to be more serious than the disease itself. The condition manifests few symptoms. However, when one falls, the weakened bone is more likely to shatter. Accordingly, the prevention and treatment of osteoporosis is critical in terms of the quality of life for postmenopausal women.
The primary goal of osteoporosis treatment is to prevent osteoporosis by ensuring peak bone mass. When osteoporosis is diagnosed, the goal is to reduce the occurrence of fracture by increasing bone density. Reproductive hormones, calcium intake, and the mechanical load are the main factors of controlling the bone regeneration activity. In case of hypoestrogenism, hormone replacement therapy can improve the symptom. As a type of anti-absorbent therapies, hormone replacement therapy can inhibit bone loss that appears in the majority of postmenopausal women. In recent years, a variety of anti-absorbent therapies have been used. They include diphosphate such as alendronate (Fosamax) as well as selective estrogen receptor modulators such as calcitonin and raloxifene (Evista), which is a new drug therapy [2,3].
Alendronate is a bisphosphonate preparation for the treatment of osteoporosis. Bisphosphonate, which is absorbed into bones and activated, reduces the number and activity of osteoclasts as well as decreases bone turnover by inhibiting apoptosis of bone cells and osteoblasts. That is also reported to reduce bone resorption and bone loss [4]. However, previous studies indicate that bisphosphonate formulation still has a lot of problems to be solved. They include a low compliance and duration; reduced effect of the drug on increasing bone mineral density as well as reducing bone turnover and fracture risks because of a higher rate of premature discontinuation [5,6]. As an interest in natural products has increased recently, attempts to analyze the effects of isoflavones, which is extracts of soy protein, have been made as estrogen replacement therapy. Soy bean has been the main food in Asia for many years, including 36 percent of protein, 18 percent of fat, 30 percent of carbohydrate, isoflavones, and a number of minerals and vitamins. It consists of eight essential amino acids and complex proteins. Isoflavones are considered as food that can replace hormone therapy as they have the structure and biological effects which are similar to those of 17-╬▓ estradiol [7]. It has been reported that isoflavone intake has a positive impact on bone metabolism [8,9], blood lipids [10,11], and body fat distribution [12] for menopausal women and ovariectomized rats. In addition, exercise therapy is known to be the most economical and effective treatment, particularly weight-bearing exercise is reported to be effective against osteoporosis [13-15]. Resistance exercise is known to have a positive impact on the maintenance and improvement of bone density. By strongly contracting and relaxing skeletal muscles, this increases muscular strength which in turn increases bone stress and contributes to bone compactness. [16]. However, it seems less feasible that Korean adult women, who do not have much experience with exercise and whose participation is low, perform resistance exercise to improve bone density. Therefore, it is believed that if the effects of weight-bearing exercise, such as walking, which can easily be practiced in real life, are compared to resistance exercise and analyzed, realistic guidelines for osteoporosis prevention and treatment can be provided.
This study is aimed at proposing the most appropriate method to treat osteoporosis which requires long-term treatments. For this, soy protein, one of estrogen replacement therapies, and alendronate which is anti-absorbent was given to rats whose menopause was induced by the removal of an ovary to compare and analyze the effects of them. In addition, this study will provide scientific data that is useful for students majoring in physical education to research matters related to bone metabolism. This can be done most directly by comparing and analyzing bone metabolism variables based on exercise methods.
METHODS
Experimental animals
In this study, sixty eight-week-old Sprague-Dawley female rats were raised for a week in advance to the experiment to help them adapt to the new environment, and after they were randomly divided into one of the four groups consisting of 10 in each group (Sham-Sedentary; SS, ovariectomized-control; OC, ovariectomized-soy protein; OS: ovariectomized-alendronate; OA, ovariectomized-endurance exercise; OE, ovariectomized-resistance exercise; OR), the surgery was conducted. After one week of recovery following the surgery, the treatment was given for the next 8 weeks. For the daily light and dark period cycle, the photoperiod consists of 12 hours of light and 12 hours of darkness. During the experiment, rats were left to freely consume the water and feed (carbohydrate: 65.4%, fat: 11.5%, protein: 22.1%, others: 1.0%, Samyang Corporation). The indoor temperature was maintained at 22 ┬▒ 2Ōäā with the humidity at 45.5 ┬▒ 5% and the daily photoperiod of 12 hours.
Surgery method
For the ovariectomy, 70 mg/kg of ketamine and 10 mg/kg of Xylazine (JW Pharmaceutical, Korea) were administered into the abdominal canal, and then the surgery site was disinfected with a 10% Betadine solution. After approximately 1.5 cm of the skin and the abdominal cavity and muscles were incised, the ovaries were exposed. After the oviduct was ligated with a silk thread, the ovariectomy was carried out on both sides. And then, the abdominal muscles and cavity and the skin were sutured with a silk thread. For the SS group, the same procedures were used only for the incision of the abdominal cavity, and the shame surgery in which the incised tissues were sutured without removing the ovaries was conducted.
Additional intake & exercise treatment method
0.4 mg of Alendronate (MARVIL 10 mg, Yuyu Inc, Korea) per kg of body weight and 200 g of isoflavones (Wisconsin, USA) per kg of feed made from bean protein extracts were mixed with the animal feed and were given to the experimental animals [17]. The exercise treatment consists of a resistance exercise and an endurance exercise. Based on the resistance exercise method suggested by Notomi, et al. [18], the study first removed the ovaries of rats and raised them in a self-made steel cylinder cage (height: 2 m, diameter: 20cm). Each cage has two water bottles which were gradually elevated until it was placed at the top of the cylinder cage, and a climbing exercise in which the rats were induced to voluntarily climb up and down the cage was conducted for 8 weeks. The endurance exercise was done first for 10 minutes per day at the speed of 10 m/min using the method suggested by Simi, et al. [19]. After the adaption period was finished, the speed and time were increased on a gradual basis. After the two weeks, the endurance exercise was done at a speed of 20 m/min for 60 minutes per day and five times per week.
Analysis method
The body weight and experimental diet intake were measured between 10 and 11 oŌĆÖclock in the morning every other day, and an electronic scale (Mettler PJ6, German) was used to calculate the weight to one-tenth of a kilogram. To measure the bone metabolism-related indexes, rats were left under fasting for 8 hours after an 8 week-long program was conducted. And then 70 mg/kg of ketamine and 10 mg/kg of Xylazine (JW Pharmaceutical, Korea) were injected into the abdominal cavity. After that, an anesthesia was administered, and the dual energy x-ray absorptiometry (DSC-3000, Aloka, Tokyo, Japan) was used to measure the body fat mass, bone mineral density (BMD; mg/cm2) and bone mineral content (BMC; mg). The blood was drawn from the inferior vena cava after the tissue was removed, which was later added with an anticoagulant, and was stirred at a rate of 3,000 rpm for 20 minutes to extract the blood plasma. The extracted blood plasma was stored in a refrigerator at a temperature of -70Ōäā until it was analyzed.
Blood variable analysis
Osteocalcin, a bone formation marker, was measured by the one-step competitive radioimunoassay using MYRIA kit (TECHNO GENETICS, Italy), and the blood estradiol level was gauged using the ELISA kit (Mercodia AB, Uppsala, Sweden).
Data analysis
All data was analyzed using the SPSS 12.0 program and was presented as the average and standard deviation of each group. To compare the parameters of all test items, the one-way ANOVA was used. The Tukey method was used for the post hoc analysis, with the significance level of p < .05.
RESULTS
Changes in body weight and body fat percentage due to additional intake treatment
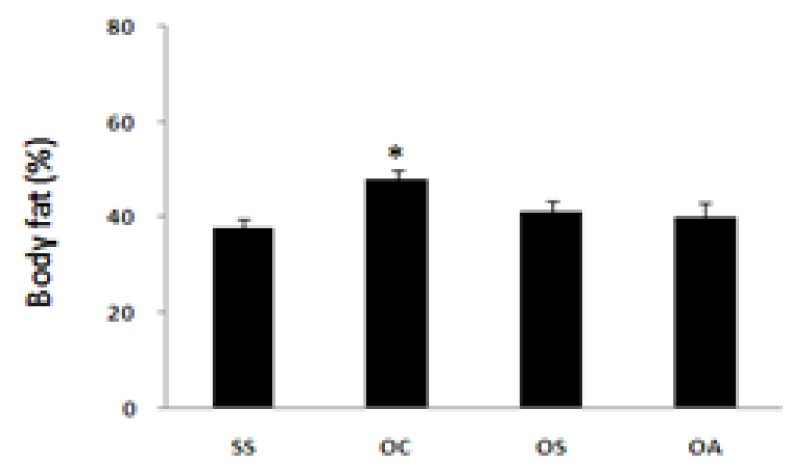
Ovariectomy increased the body weight and body fat percentage like menopause, while the 8 week-long bean protein diet and the alendronate treatment did not influence the body weight. However, the 8 week-long bean protein diet and the alendronate treatment suppressed an increase in the body fat percentage (p < .05, Fig. 1, 2).
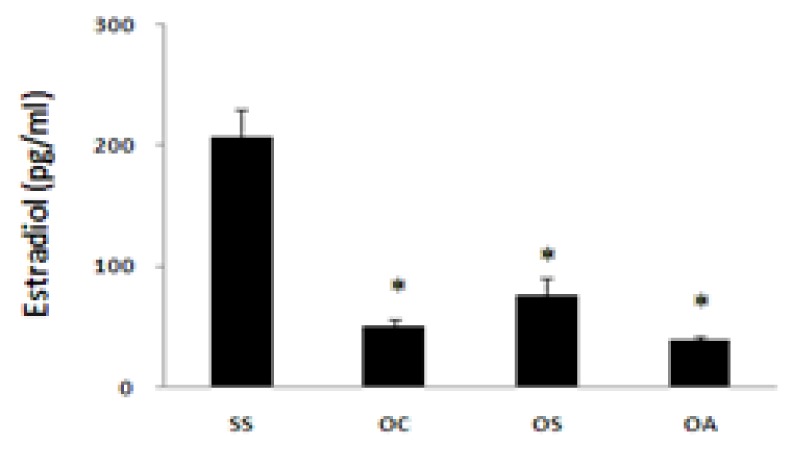
Changes in blood estradiol and osteocalcin due to additional intake treatment
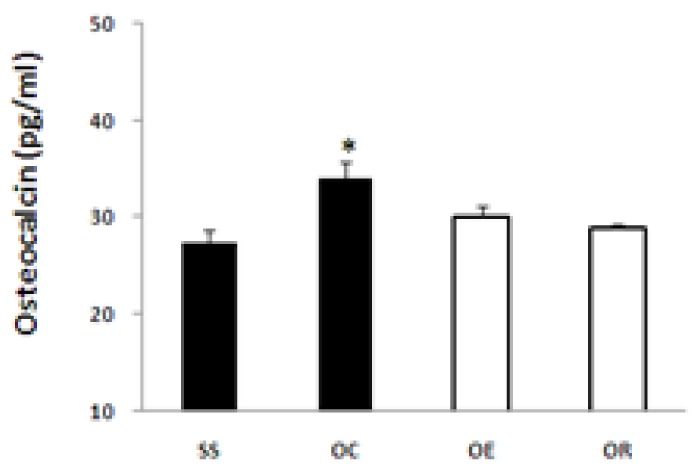
The ovariectomy on the eight-week-old Sprague-Dawley female rats lowered the blood estradiol (E2) by four times (p < .05), while the 8 week-long bean protein diet and the alendronate treatment did not influence the blood estradiol level (Fig. 8). Those rats which experienced the menopause induced by ovariectomy showed a significant increase in the blood osteocalcin level compared with the SS group (p < .05). The 8 week-long bean protein diet and the alendronate treatment significantly decreased the blood osteocalcin level (p < .05). Especially, the alendronate treatment reduced the osteocalcin level to lower than the SS group (p < .05).
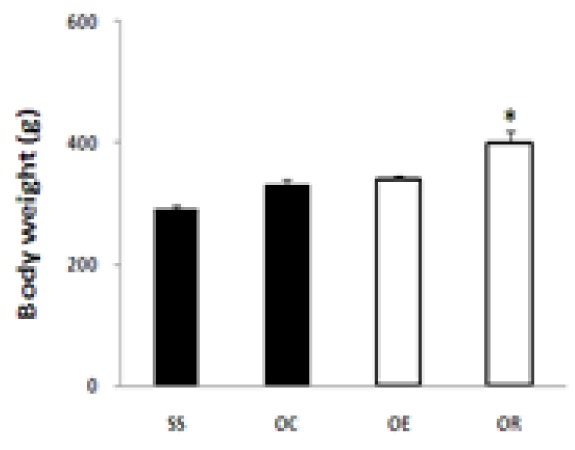
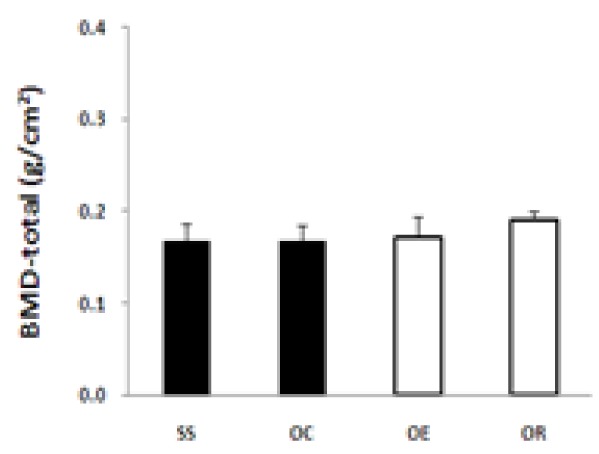
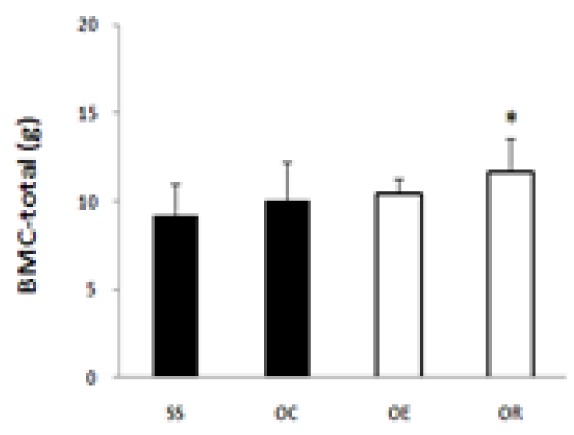
Changes in the body weight, bone density and blood osteocalcin depending on the type of exercise
The 8 week-long low intensity treadmill running did not influence the body weight, bone density and bone mass. However, the 8 week-long climbing exercise significantly increased the body weight and bone density (p < .05, Fig. 10~12). The 8 week-long exercise treatment showed a tendency of reducing the blood osteocalcin level which was previously increased by the ovariectomy, but failed to indicate a statistical significance (Fig. 13).
DISCUSSION
Women usually undergo many changes caused by the menopause, and among them, the most typical diseases resulting from an estrogen deficiency include cardiovascular diseases and osteoporosis. Especially, osteoporosis is a disease that does not have a direct impact on the body but can cause a fracture which can substantially worsen the quality of life. Therefore, the prevention and treatment of osteoporosis is very important in ensuring the quality lives of women. To prevent and treat the osteoporosis, a medication, exercise and additional intake treatment are commonly used. However, except for the diet regimen, the medication and exercise treatment are often faced with problems such as a low adaption rate and a low continuation rate. These problems occur due to environmental difficulty, as the mechanism and efficacy of these treatments have not been clearly confirmed yet. Therefore, this study aimed to present a clear guideline in the prevention and treatment of osteoporosis by comparing the commonly used medications and exercise treatments, and to offer the most suitable treatment solution for osteoporosis, which requires a long period of treatment, by identifying the most effective treatment in combination with an exercise or a medication treatment. To this end, the most typical medication, alendronate, was administered and the bean protein diet, one of the most widely used alendronate and estrogen alternative therapy, was given to the rates with menopause induced by ovariectomy in order to compare their efficacies. As an exercise therapy, the treadmill running was used for the endurance exercise, while the climbing exercise was adopted for the endurance test.
According to the study results, the ovariectomy reduced the blood estradiol level by 4 times. There are three types of estrogen such as estrone, estradiol and estriol. Estradiol is a major blood estrogen, which is dominant before menopause, and can be dramatically reduced when the ovaries are removed [20]. According to Monroe, et al. [21], it was reported that the estradiol concentration in the blood plasma was immediately decreased and the estradiol concentration in the blood plasma was reduced to 20pg/ml. Based on these results, the study believed that the menopause induced by ovariectomy was successful. In case of menopause, the influence of androgen increases, bringing about a negative effect on the physiology of women such as an increase in visceral fat accumulation and abdominal obesity [22]. And the study observed a significant increase in the body weight and the body fat percentage. However, the 8 week-long bean protein diet and the alendronate treatment did not influence the diet intake and body weight but suppressed an increase in the body fat percentage. This was consistent with the previous study results that the intake of food containing soy protein can significantly reduce the body weight, BMI, body fat percentage, and the alendronate treatment contributed to weight loss and a decrease in the body fat percentage through the control of food intake and the acceleration of energy metabolism and lipid oxidation [23-25].
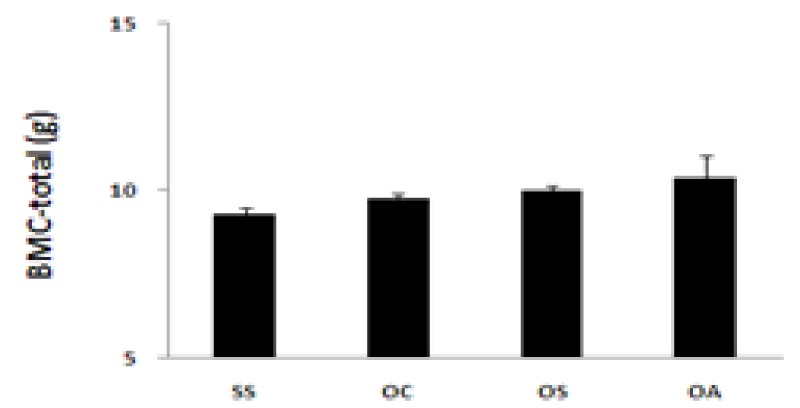
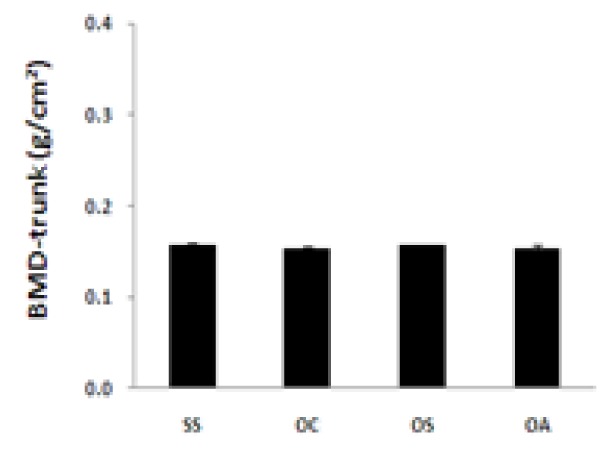
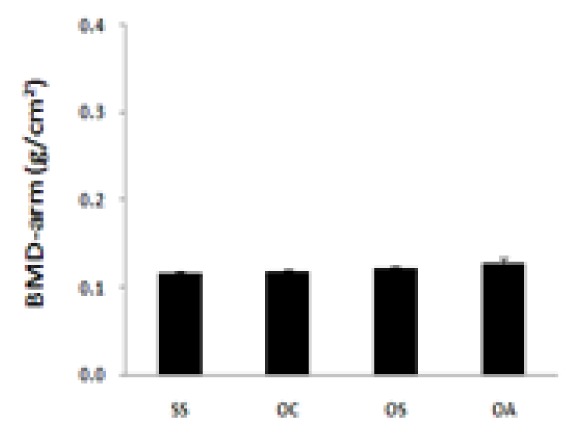
In terms of changes in the bone density, the results are contrary to the earlier expectation. The 8 week-long bean protein diet and the alendronate treatment did not have a significant influence on the total bone density and total bone mass as well as the regional bone density in the upper and lower limbs and the trunk, while the ovariectomy did not lead to a decrease in the bone density. However, the blood osteocalcin level was increased by about 30% due to the ovariectomy, while the bean protein diet and the alendronate treatment decreased the blood osteocalcin level. Especially, the alendronate treatment significantly decreased the blood osteocalcin level. This was consistent with the previous study findings that the blood osteocalcin level in ovariectomized rats increased as it does in case of menopause [26,27]. Osteocalcin was closely bonded with hydroxyapatite and calcium in the bone structure, and was known as a bone formation marker to predict the bone loss rate, because it is indirectly engaged in the activation of osteoblasts in case of the formation of a new bone [28,29]. However, although this study showed a positive change in the bone metabolism index, it failed to have a significant influence on the bone density. This is because the experiment period of this study (8 weeks) was relatively shorter than the previous studies (18 weeks).
To establish a guideline for an exercise effective in preventing and treating osteoporosis, the parameters were compared and analyzed by administering the 8 week-long voluntary climbing exercise or low-intensity treadmill exercise. The study results showed that a low intensity endurance exercise significantly increased the body weight and bone mass compared with the voluntary climbing exercise. However, the increased blood osteocalcin level due to the ovariectomy was reduced again in both the endurance exercise and climbing exercise. It has been believed so far that the body-weight-supported resistance exercise is the most effective in improving the bone density as it can help develop the muscle strength and the muscle system. In fact, a multitude of studies observed that the resistance exercise can improve the bone density [30,31] and that an exercise requiring a high intensity muscle strength and impact stress is known to increase the bone quantity more than an endurance exercise. However, the exercise type should be determined in consideration of age and physical limitations of a group or an individual. This study indicated that the influence of a low intensity endurance exercise on the blood osteocalcin level was similar to a resistance level. Although it failed to lead to an increase in the bone density, it was thought that a long period of exercise treatment could bring about more intriguing results. However, both types of exercises did not show a significant change in the bone density except for the bone mass, and as a result, all treatments were not good enough to show any meaning effects. This was not because these treatments were not effective at all. It is believed that there is a need to apply the concept of dose-response relationship. In addition, there is a possibility that a mutually compensatory mechanism was in the work in relation to these changes. There is a need to focus on a possibility that a multitude of mechanisms are activated to compensate for each other when the treatment effect did not show any significance.